
Metabolic dysfunction-associated steatotic disease (MASLD) used to be called nonalcoholic fatty liver disease. Metabolic dysfunction-associated steatotic disease (MASLD) is the most common cause of chronic liver disease in Western countries around 20-30% that is predicted to become also the most frequent indication for liver transplantation by 2030. Metabolic dysfunction-associated steatotic disease (MASLD) is a broad term used to cover a spectrum of conditions that are characterized by evidence of hepatic steatosis on imaging or histology (macro-vesicular steatosis), and absence of secondary causes of hepatic steatosis such as significant alcohol consumption, chronic use of medications that can cause hepatic steatosis or hereditary disorders. Metabolic dysfunction-associated steatotic disease (MASLD) is most often diagnosed incidentally on imaging or when it presents with complications. MASLD is considered to be the liver manifestation of metabolic syndrome. 50 to 70% of people with diabetes are found to have MASLD.
Over the last decade, it has been shown that the clinical burden of MASLD is not only confined to liver-related morbidity and mortality, but there is now growing evidence that MASLD is a multisystem disease, affecting extra-hepatic organs and regulatory pathways. For example, MASLD increases risk of type 2 diabetes mellitus (T2DM), cardiovascular (CVD) and cardiac diseases, and chronic kidney disease (CKD). Although the primary liver pathology in MASLD affects hepatic structure and function to cause morbidity and mortality from cirrhosis, liver failure and hepatocellular carcinoma, the majority of deaths among MASLD patients are attributable to CVD.
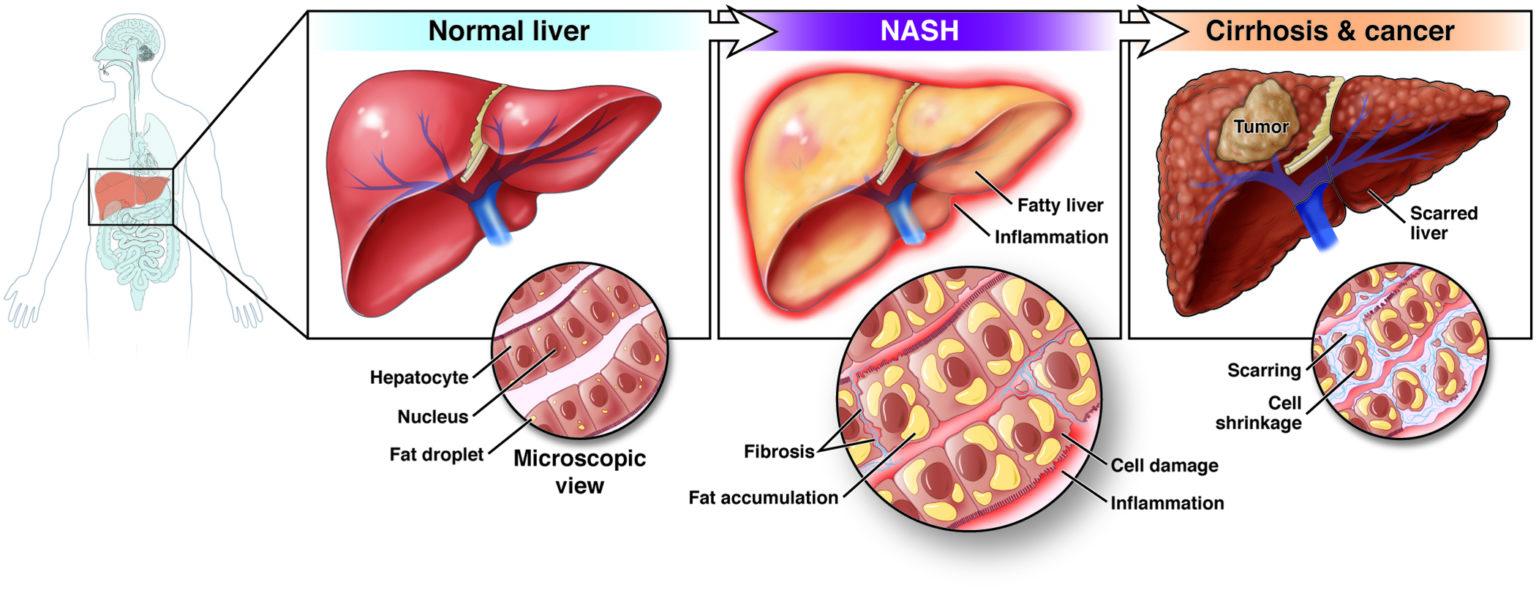
MASLD has several phases of progression, which include simple steatosis, steatohepatitis, fibrosis, cirrhosis, and ultimately could even progress to hepatocellular carcinoma. The disease has a benign course; it is a silent liver disease when the only histological finding is steatosis. The presence of hepatic injury with inflammation with or without fibrosis constitutes non-alcoholic steatohepatitis (NASH).
Metabolic dysfunction-associated steatohepatitis (MASH) is a more severe form of MASLD characterized by inflammation and liver damage, including fibrosis (scarring). NASH causes the liver to swell and become damaged due to the fat deposits in the liver. NASH may get worse and may lead to serious liver scarring, called cirrhosis, and even liver cancer. This damage is like the damage caused by heavy alcohol use.
There are several different scales of liver fibrosis staging, where a doctor determines the degree of liver damage. This may be achieved with a variety of methods, such as blood work, imaging tests, and a tissue biopsy that may be further examined under a microscope (histology).
But first, a doctor will need to diagnose any underlying chronic liver disease, such as fatty liver disease or hepatitis. This can help identify the underlying causes of inflammation that lead to fibrosis, and better guide the staging and treatment process. While fibrosis staging can help the patient and a doctor understand the degree to which your liver might be damaged, it’s important to note that the identifying the underlying cause is more important than focusing on any particular stage. If a liver biopsy and histology is performed, a doctor may stage liver fibrosis based on the METAVIR scoring system. This assigns a “score” based on two factors: inflammation (activity) and damage (fibrosis). A lower score may indicate less inflammation and damage, while a higher score could mean more.
The activity grades range from A0 to A3:
A0: no activity
A1: mild activity
A2: moderate activity
A3: severe activity
The fibrosis stages range from F0 to F4:
F0: no fibrosis
F1: portal fibrosis without septa
F2: portal fibrosis with few septa
F3: numerous septa without cirrhosis
F4: cirrhosis
Therefore, a person with the most severe disease form may have an A3, F4 METAVIR score.
Another scoring system based in histology is Batts and Ludwig, which grades fibrosis on a scale of grade 1 to grade 4, with grade 4 being the most severe.
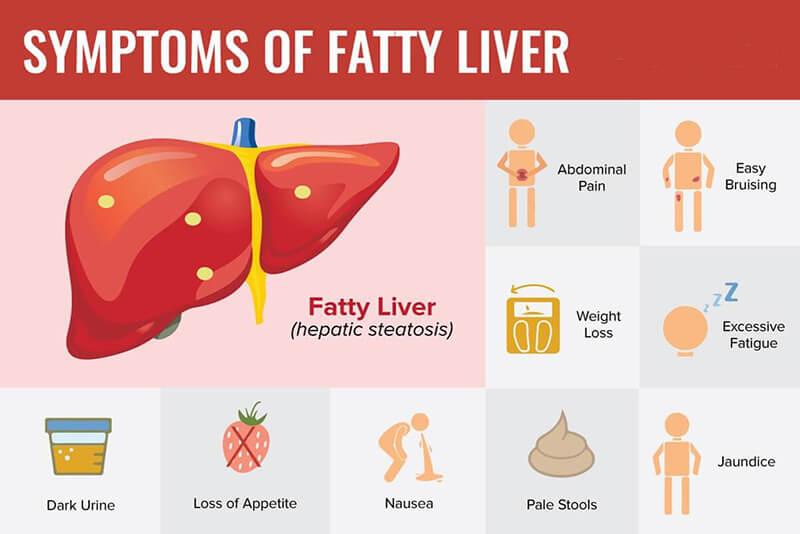
MASLD is sometimes called a silent liver disease. This is because it can happen without causing any symptoms. Most people with MASLD live with fat in their liver without getting liver damage. A few people who have fat in their liver develop metabolic dysfunction-associated steatohepatitis (MASH).
Symptoms from MASH may include:
MASH that turns into cirrhosis could cause these symptoms:
How to Diagnosed Metabolic dysfunction-associated steatotic disease (MASLD)?
Metabolic dysfunction-associated steatotic disease (MASLD) can happen without causing any symptoms. It’s often diagnosed when someone have routine blood test to check liver. The condition is typically diagnosed after a blood test finds higher than normal levels of liver enzymes. A standard blood test could reveal this result.
The healthcare provider may use these tests to help make a diagnosis:
Risk Factor
Children and young adults can get this disease. But it is most common in middle age. Risk factors include:
When these risk factors happen together, they cause a health problem called metabolic syndrome. People with metabolic syndrome often have fatty liver. They also are more likely to have heart disease. Other conditions that may raise your risk include polycystic ovary syndrome, sleep apnea, and hypothyroidism.
Complications
The primary risk of MASH is progressive fibrosis leading to cirrhosis of the liver. This occurs in 5% to 12% of people with MASH.
Cirrhosis is associated with an increased risk of liver cancer. Most people with liver cancer have cirrhosis. MASLD and MASH are also both associated with an increased risk of cardiovascular disease and Type 2 diabetes. It works both ways: having these conditions makes you more likely to have metabolic dysfunction-associated steatohepatitis, and vice versa.
Manage the blood lipid levels by maintaining a weight, that’s healthy for patient with MASH, reducing cholesterol in the diet and managing blood sugar. Get a little exercise. Avoid carcinogens such as tobacco smoke.
Treatment
Until recently, there were no medications that could treat MASH. Additional guidelines include:
Home remedies includes:
a. Silymarin
Herbal products are increasingly used, mainly in chronic liver disease like Silymarin. Silymarin is a complex of at least seven flavonolignans that are the most common class of compounds present in milk thistle extract, and one flavonoid, Taxifolin. Silybin represents about 50% to 70% of the silymarin extract. Experimental studies have clearly demonstrated the antifibrotic, antioxidant and metabolic effects of silybin. The antioxidant effects of Silybin have been demonstrated in all cells studied.
Silybin acts as an antioxidant because it inhibits radical formation, binds some radical species (scavenger), interferes with lipid peroxidation of membranes (and therefore modulates membrane permeability), and increases the intracellular content of scavengers. In fact, in the presence of oxidative and nitrosative stress, silybin inhibits the formation of superoxide anion radicals and nitric oxide (NO), increases ATP content through the phosphorylation of ADP, decreases the content of malondialdehyde (MDA) and totally abolishes the decrease of glutathione, of superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase.
Flavonolignans like Silymarin or Silybin are known for their poor and erratic bioavailability, low solubility in water, and poor intestinal absorption. To counteract this aspect, different more soluble derivates of silybin have been synthesized, such as silybin-phosphatidylcholine. Bioavailability of Silybin-Phosphatidylcholine is higher than that of silymarin and is less influenced by liver damage.
b. Folate
Folate, also known as vitamin B9, plays a crucial role in various bodily functions, including DNA synthesis and repair, red blood cell formation, and homocysteine metabolism. In particular, in several animal studies, low folate levels have been linked to oxidative stress, liver damage, and hepatocarcinogenesis. Folate plays an important role in regulating hepatic metabolism.
Folate deficiency can result in elevated homocysteine levels, a risk factor for cardiovascular diseases, which are common comorbidities in patients with liver disease. Folate supplementation may be beneficial for patients with liver disease to prevent or correct deficiencies. This can help mitigate of the associated risks, such as elevated homocysteine levels.
PT. SIMEX PHARMACEUTICAL INDONESIA as one of the pharmaceutical companies in Indonesia presents HEPARLIC® products as a herbal medicine contain the newest combination of Silybin-Phosphatidylcholine Complex, the active form of Silymarin and 5-MTHF as a biologically active form of folic acid. HEPARLIC® can help to support liver health because of its effects as an antioxidant and antifibrotic.
Reference
Grander C., Grabherr F., Tilg H. 2022. Non-alcoholic fatty liver disease: pathophysiological concepts and treatment options. Cardiovascular Research (2023) 119, 1787-1798.
Loomba R., Friedman SL., Shulman GI. 2021. Mechanisms and disease consequences of nonalcoholic fatty liver disease. Cell 184, May 13,2021.
Huh Y., Cho YJ., Nam GE. 2022. Recent Epidemiology and Risk Factors of Nonalcoholic Fatty Liver Disease. Journal of Obesity & Metabolic Syndrome 2022; 31:17-27.
Byrne CD., Targher G. 2015. NAFLD: A multisystem disease. Journal of Hepatology 2015 vol. 62 S47-S64
Pouwels S., Sakran N., Graham Y., et.al. 2022. Non-alcoholic fatty liver disease (NAFLD): a review of pathophysiology, clinical management and effects of weight loss. BMC Endocrine (2022) 22:63.
https://www.hopkinsmedicine.org/health/conditions-and-diseases/nonalcoholic-fatty-liver-disease
https://www.healthline.com/health/nonalcoholic-fatty-liver-disease#diagnosis
https://patient.gastro.org/mafld-mash/
https://www.healthline.com/health/liver-fibrosis#stages
https://www.nash24x7.com/non-alcoholic-fatty-liver-disease-causes-symptoms-treatments/








